Clinical Assessment and Treatment Form Template - Documenting Care for Outpatient Patients
Outpatient clinicians frequently struggle with the administrative burden of documenting complex patient care accurately without compromising valuable face-to-face treatment time. As insurance reimbursements and federal Medicare funding increasingly depend on rigorous compliance metrics, structured documentation has become a non-negotiable necessity for clinic survival.
This essential patient power tool-the Clinical Assessment and Treatment Form Template-grants practitioners immediate operational relief by streamlining clinical intake. Please note the educational stipulation: while this template optimizes workflow efficiency, it is designed to support, not replace, individualized clinical judgment.
For example, outpatient clinics utilizing standardized assessment templates, such as physical therapy departments tracking specific Range of Motion (ROM) progress, report a substantial reduction in billing audit risks. Below, we will explore how to effectively integrate this template into your daily workflow to elevate outpatient care standards.
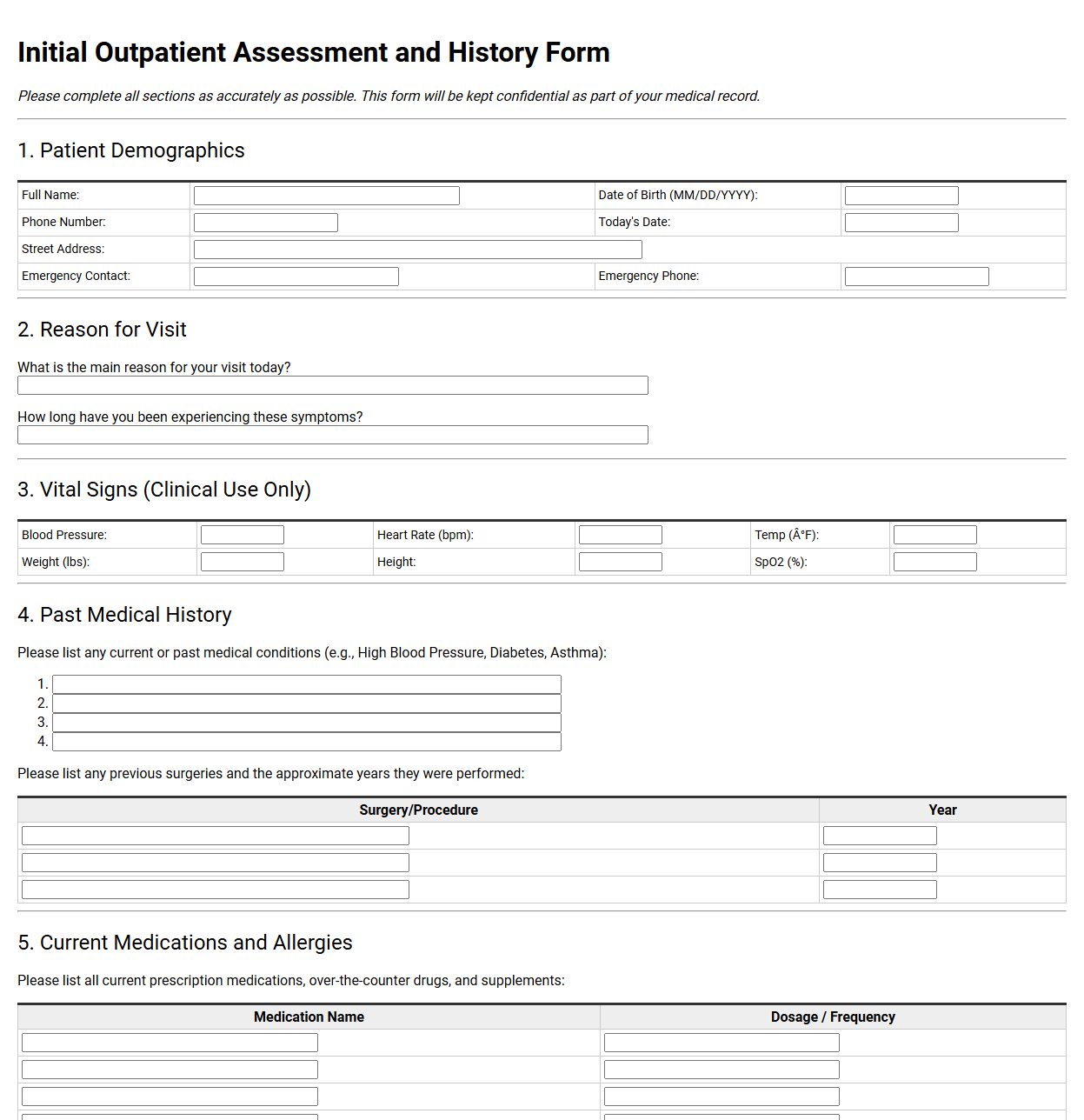
Initial Outpatient Assessment and History Form
💾 Initial Outpatient Assessment and History Form .pdf
The initial outpatient assessment and history form gathers crucial baseline data before clinical treatment begins. This document records patient demographics, current medical concerns, past surgeries, and family health backgrounds. It also tracks allergies, active medications, and lifestyle habits, ensuring healthcare providers can design safe, highly personalized patient care plans.
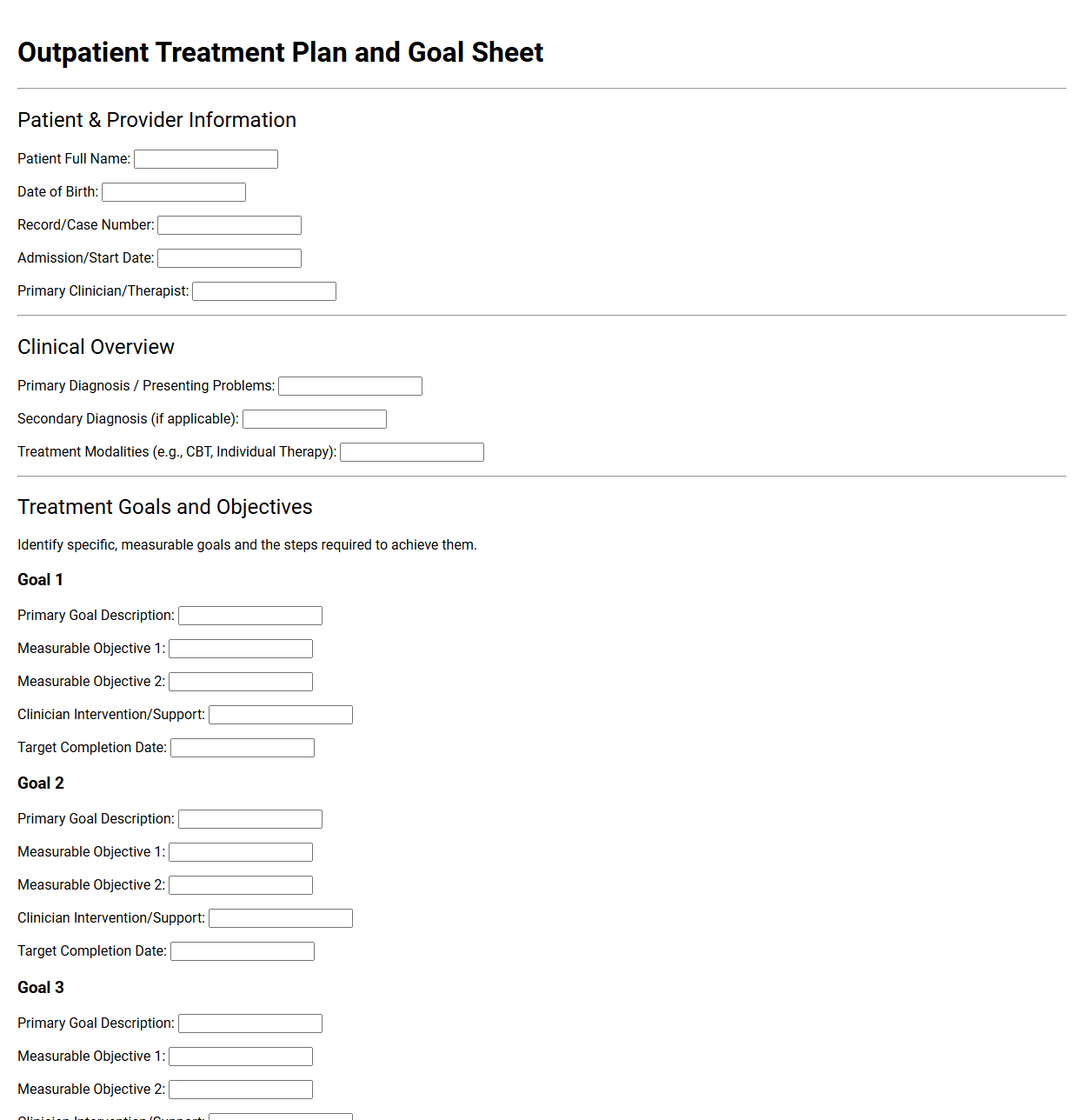
Outpatient Treatment Plan and Goal Sheet
💾 Outpatient Treatment Plan and Goal Sheet .pdf
An outpatient treatment plan and goal sheet outlines a patient's therapeutic journey. This structured document details specific, measurable objectives, planned interventions, and target dates. It serves as a collaborative roadmap between clinicians and clients, tracking progress and milestones for recovery while ensuring accountability and clear communication throughout the clinical process.
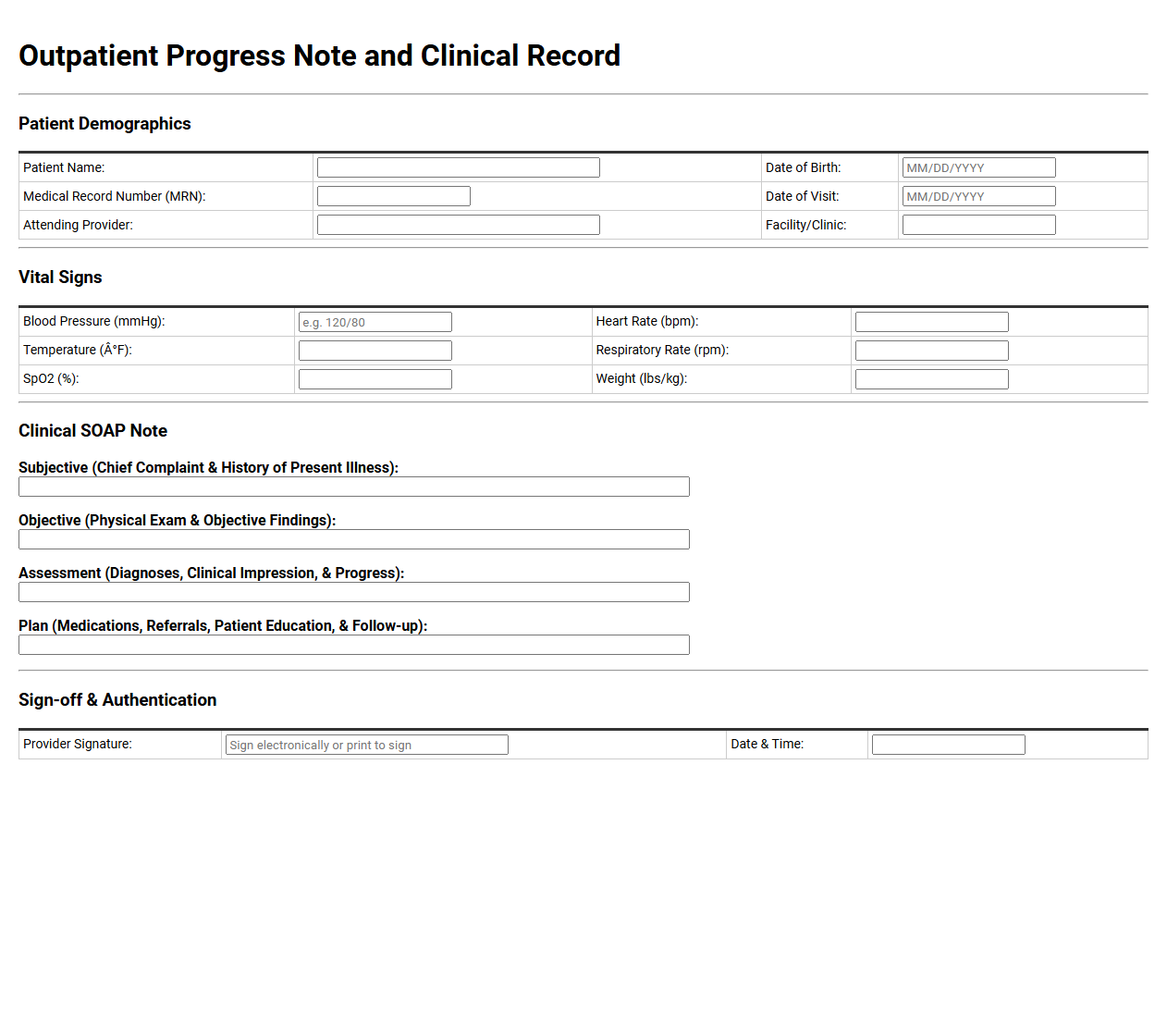
Outpatient Progress Note and Clinical Record
💾 Outpatient Progress Note and Clinical Record .pdf
An outpatient progress note documents a patient's clinical encounter, detailing the chief complaint, vital signs, physical examination findings, and diagnostic assessments. This clinical record tracks treatment efficacy over time, guides subsequent medical decisions, and facilitates clear communication among healthcare providers to ensure continuous, safe, and highly coordinated overall patient care.
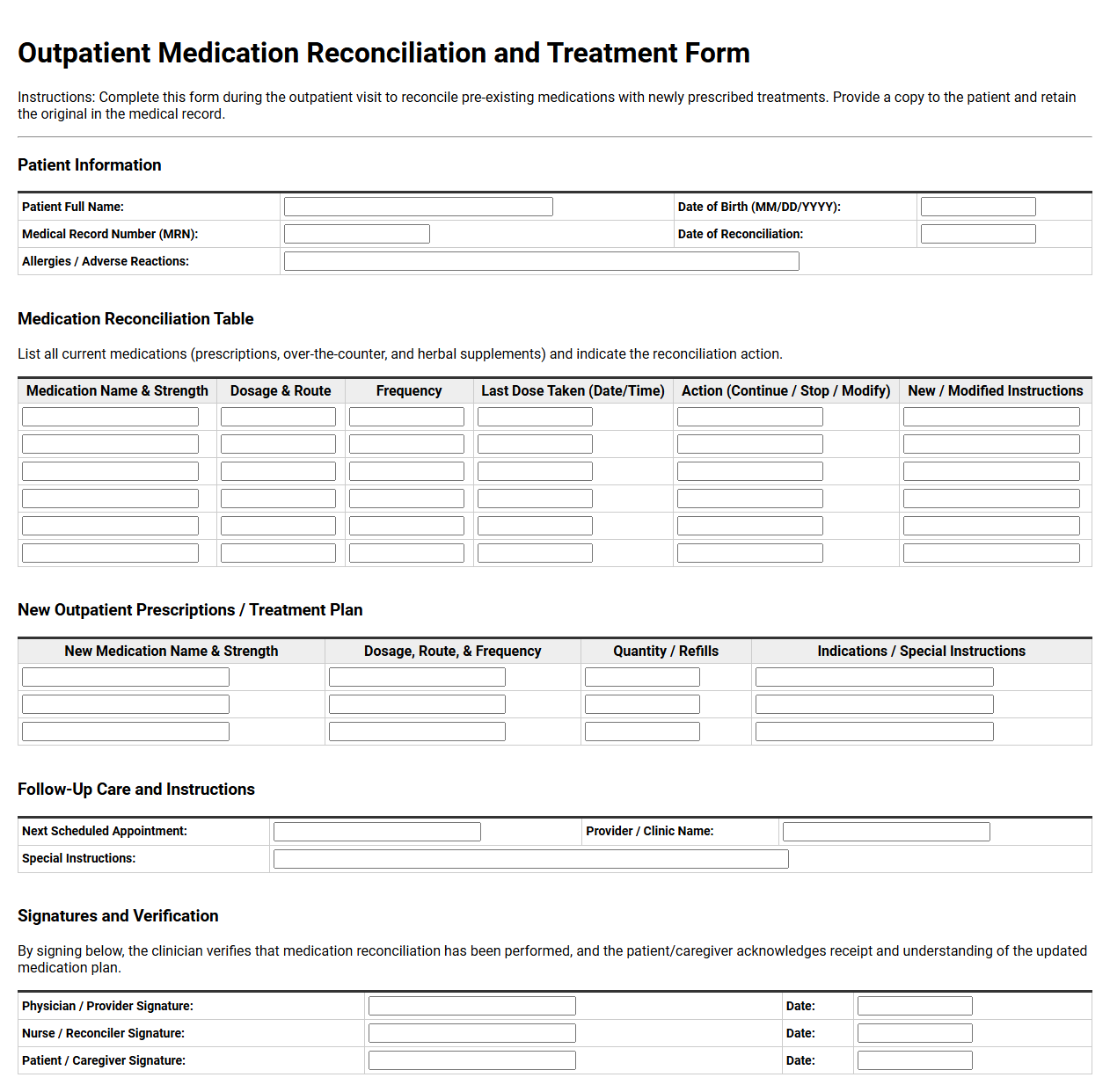
Outpatient Medication Reconciliation and Treatment Form
💾 Outpatient Medication Reconciliation and Treatment Form .pdf
An Outpatient Medication Reconciliation and Treatment Form compiles a patient's complete medication history, comparing current prescriptions with newly ordered therapies. This clinical document helps healthcare providers identify discrepancies, prevent harmful drug interactions, and establish an accurate treatment plan during outpatient visits, promoting patient safety throughout their ongoing care journey.
Patient Pain Assessment and Management Form
💾 Patient Pain Assessment and Management Form .pdf
A patient pain assessment and management form is a clinical tool used by healthcare providers to document a patient's pain levels, location, and characteristics. This document tracks pain intensity over time, evaluates the effectiveness of treatments, and helps clinicians create personalized care plans to improve overall comfort and recovery.
Outpatient Referral and Clinical Consultation Form
💾 Outpatient Referral and Clinical Consultation Form .pdf
An outpatient referral and clinical consultation form facilitates seamless communication between healthcare providers. This document captures vital patient data, clinical history, and specific reasons for specialist evaluation. It ensures accurate information transfer, streamlining the transition of care and helping specialists deliver targeted treatment recommendations promptly and safely.
Mental Health Outpatient Intake and Assessment Form
💾 Mental Health Outpatient Intake and Assessment Form .pdf
A mental health outpatient intake and assessment form gathers critical patient information before therapy begins. It documents personal demographics, medical history, current symptoms, and treatment goals. This standardized clinical document helps practitioners understand unique patient needs, identify potential risks, and design highly effective, personalized therapeutic plans for successful patient recovery.
Pediatric Outpatient Physical Assessment Template
💾 Pediatric Outpatient Physical Assessment Template .pdf
A pediatric outpatient physical assessment template provides a structured framework for clinicians evaluating children. This clinical document guides therapists through developmental milestones, motor skills, reflex integration, and sensory processing. By recording precise observations, therapists track developmental progress and design tailored intervention plans for young patients in outpatient clinics.
Outpatient Nursing Assessment and Triage Form
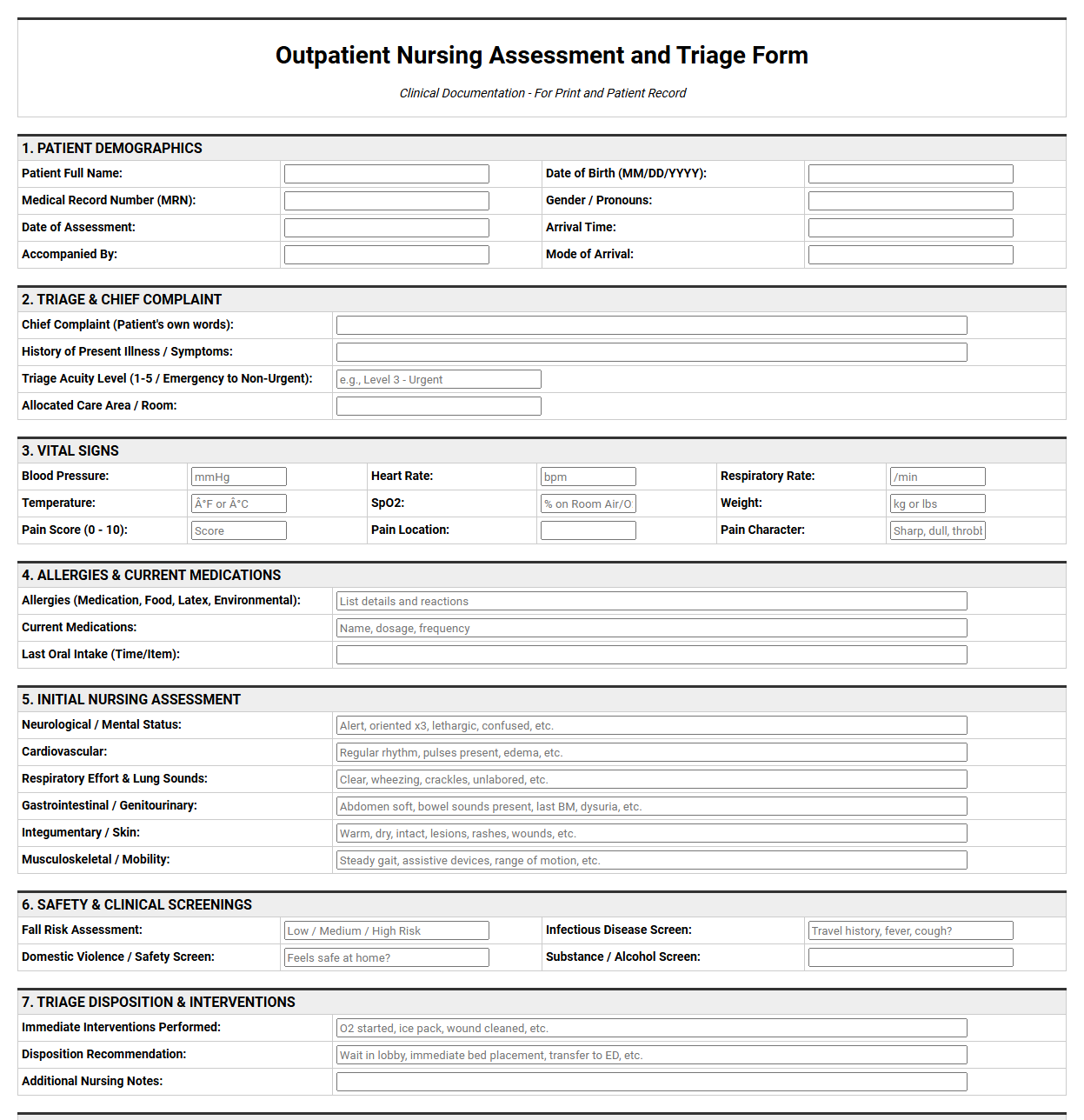
💾 Outpatient Nursing Assessment and Triage Form .pdf
An outpatient nursing assessment and triage form is a clinical tool used to record vital signs, chief complaints, and medical histories. It guides nurses in prioritizing patient care based on clinical urgency. This structured document ensures accurate data collection, facilitating safe transitions and timely medical interventions within outpatient clinics.
Physical Therapy Outpatient Evaluation and Treatment Form
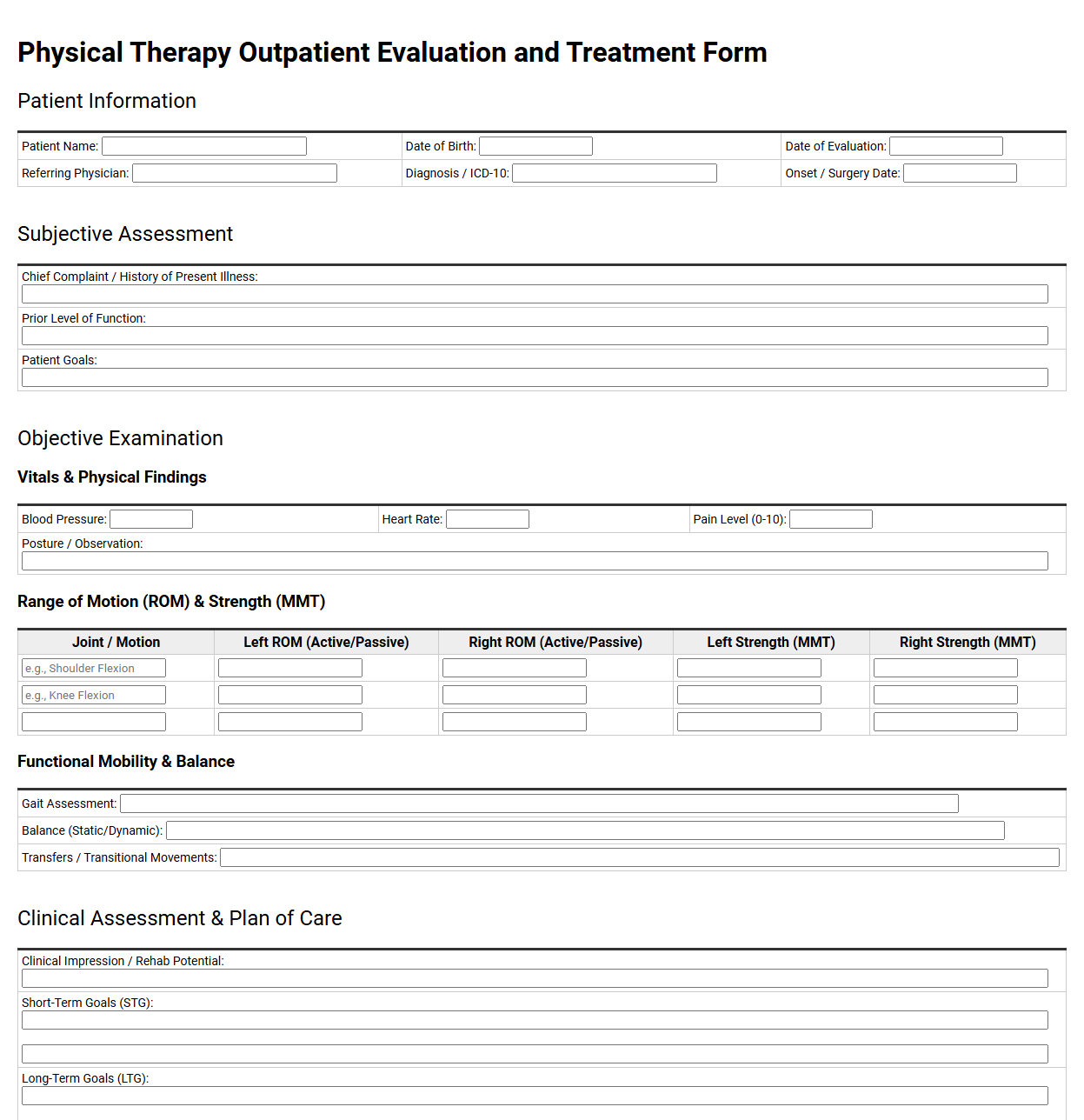
💾 Physical Therapy Outpatient Evaluation and Treatment Form .pdf
The Physical Therapy Outpatient Evaluation and Treatment Form documents a patient's initial clinical assessment and ongoing care plan. It records medical history, current pain levels, functional limitations, and objective measurements. Therapists use this structured record to establish functional goals, outline specific therapeutic interventions, and track rehabilitation progress over time.
Outpatient Discharge Summary and Aftercare Plan
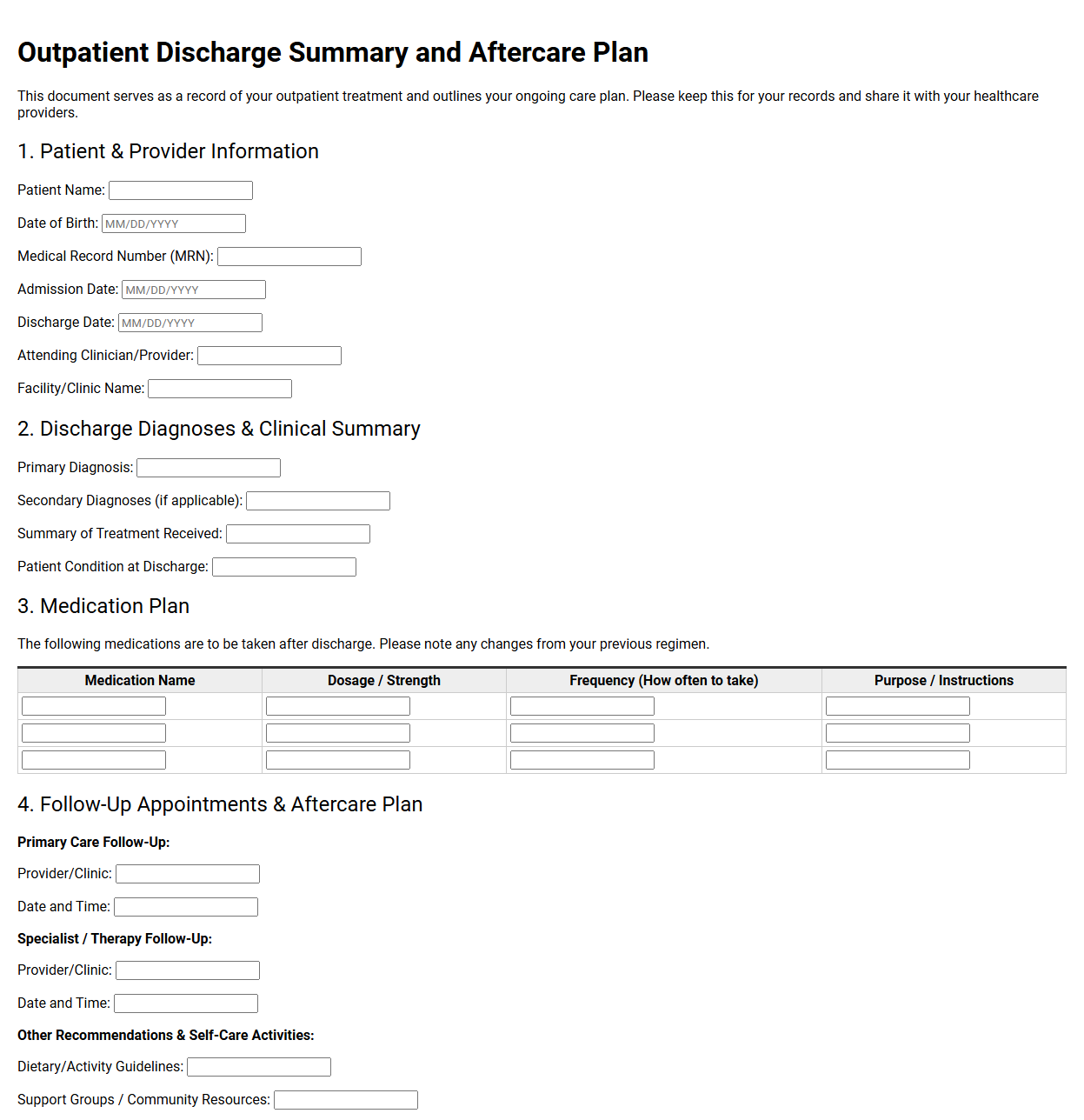
💾 Outpatient Discharge Summary and Aftercare Plan .pdf
An outpatient discharge summary and aftercare plan details a patient's transition from clinical care. This vital document records diagnoses, treatments administered, and medication changes. It outlines crucial follow-up appointments, dietary restrictions, and activity guidelines, ensuring a safe recovery and clear communication between diverse healthcare providers and the patient at home.
Follow Up Outpatient Assessment and Progress Form
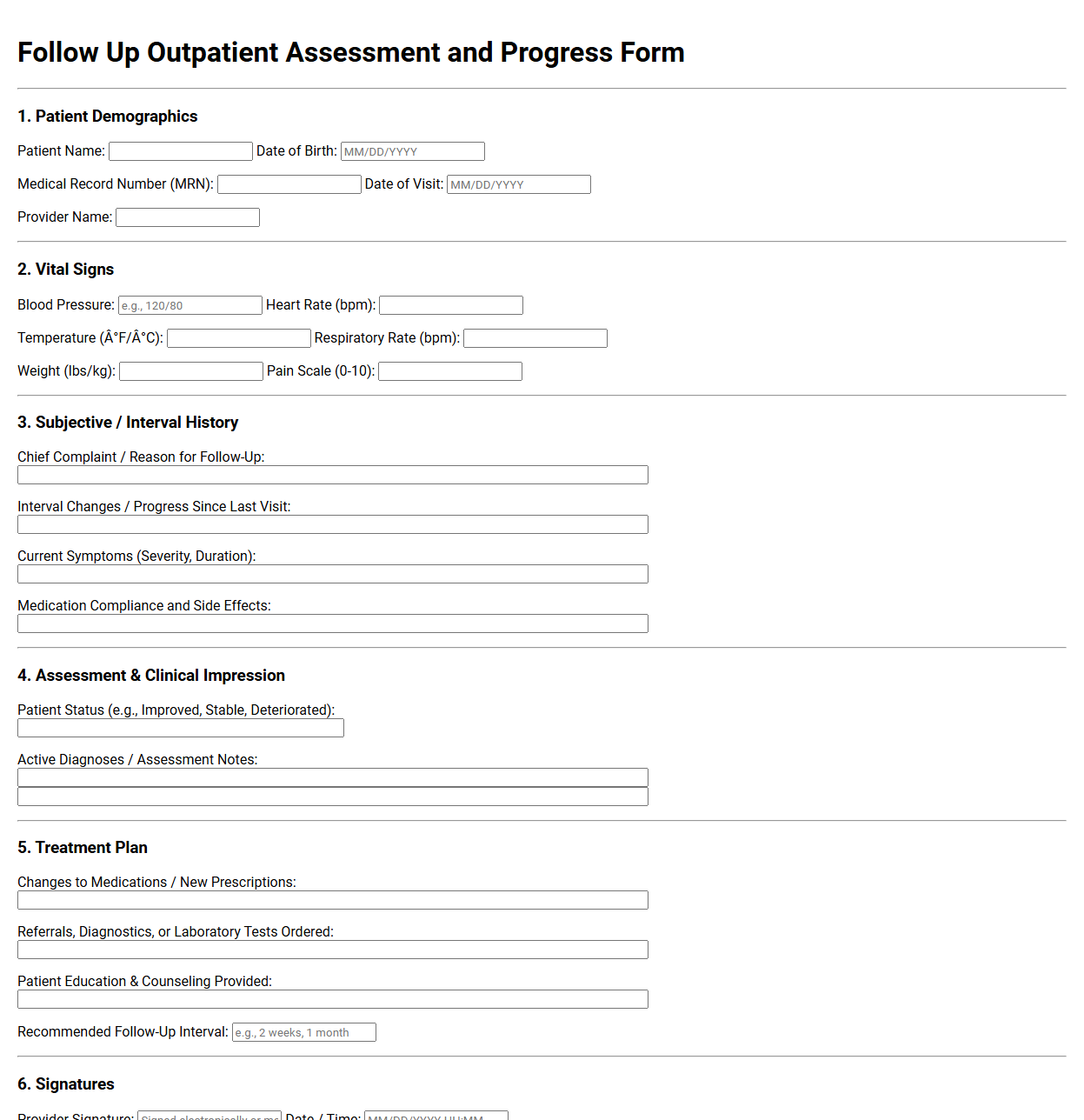
💾 Follow Up Outpatient Assessment and Progress Form .pdf
A follow-up outpatient assessment and progress form tracks a patient's recovery journey after initial treatment. This clinical document records vital signs, symptom changes, medication adherence, and ongoing therapy responses. It helps healthcare providers update care plans, document clinical decisions, and ensure continuous, coordinated care across subsequent medical visits.
Outpatient Informed Consent and Treatment Authorization
💾 Outpatient Informed Consent and Treatment Authorization .pdf
An outpatient informed consent and treatment authorization document establishes a clear agreement between patients and healthcare providers. It outlines proposed medical procedures, potential risks, expected benefits, and alternative options. By signing, patients acknowledge their understanding of the care plan, authorize voluntary treatment, and accept financial policies and privacy practices.
Cardiology Outpatient Assessment and Treatment Record
💾 Cardiology Outpatient Assessment and Treatment Record .pdf
A cardiology outpatient assessment and treatment record compiles critical cardiovascular health data. This clinical document details patient medical history, diagnostic test results like electrocardiograms, and therapeutic strategies. It tracks cardiac symptoms, medication adjustments, and management plans, ensuring structured continuity of care during subsequent specialized clinic visits for cardiac patients.
Geriatric Outpatient Assessment and Treatment Plan
💾 Geriatric Outpatient Assessment and Treatment Plan .pdf
A typical geriatric outpatient assessment and treatment plan comprehensively details an older adult's medical history, cognitive function, and daily living capabilities. This vital document outlines personalized therapeutic interventions, medication management strategies, and support services, aiming to optimize independence, manage chronic conditions, and enhance the patient's overall quality of life.
Patient Outpatient Assessment and Treatment FAQ
What is the primary purpose of an outpatient assessment?
An outpatient assessment evaluates a patient's physical, mental, and functional status without hospital admission. It helps clinicians establish an accurate baseline diagnosis, identify immediate healthcare needs, and formulate a targeted, personalized treatment plan that allows the patient to safely return home after their scheduled clinical appointment.
What clinical components are typically evaluated during this assessment?
The assessment comprehensively covers vital signs, medical history, current symptoms, cognitive function, and lifestyle factors. Clinicians also review active medications and potential allergies. This holistic evaluation ensures that any prescribed outpatient therapies align safely with the patient's existing health profile and daily living activities.
How does outpatient treatment differ from inpatient care?
Outpatient treatment is designed for medically stable patients who do not require 24-hour monitoring. Patients receive specialized therapeutic interventions, counseling, or rehabilitation during scheduled clinical visits and return to their daily routines. In contrast, inpatient care requires overnight hospitalization for acute conditions demanding continuous medical supervision.
What role does the treatment plan play in outpatient care?
The treatment plan serves as a clinical roadmap detailing specific therapeutic interventions, medication regimens, and therapy schedules. It outlines measurable health goals, progress benchmarks, and follow-up intervals, ensuring both the healthcare provider and the patient remain aligned on the path to recovery and long-term health management.
How does the outpatient assessment facilitate continuity of care?
This assessment provides a documented clinical baseline shared across the multidisciplinary care team, including primary physicians, specialists, and therapists. By standardizing diagnosis and progress tracking, it prevents gaps in care, avoids duplicate testing, and ensures seamless communication as the patient moves through different phases of recovery.
Disclaimer:
The documents and templates provided on this page are for informational and illustrative purposes only. They do not constitute professional, legal, or financial advice, and should not be relied upon as such. Because individual circumstances and regulatory requirements vary, these materials may not be suitable for your specific needs. We recommend consulting with a qualified professional before adapting or using any of these examples for official or commercial purposes.