Patient Medical History and Health Questionnaire Template - Streamlining Patient Intake and Clinical Anamnesis
Gathering comprehensive clinical anamnesis during patient intake remains a persistent operational bottleneck for healthcare providers, often resulting in fragmented patient data and delayed care. While clinics typically rely on standard operational budgets or healthcare technology grants to finance administrative upgrades, optimizing patient-facing intake systems represents a highly cost-effective alternative.
This Patient Medical History and Health Questionnaire Template serves as a patient power tool that grants practitioners immediate, structured diagnostic insights before the patient even enters the exam room. While this digital framework is not a substitute for direct clinical examination, it has proven vital in active care environments, such as tracking chronic hypertension timelines. Below, we explore how this tool streamlines patient intake and enhances clinical documentation precision.
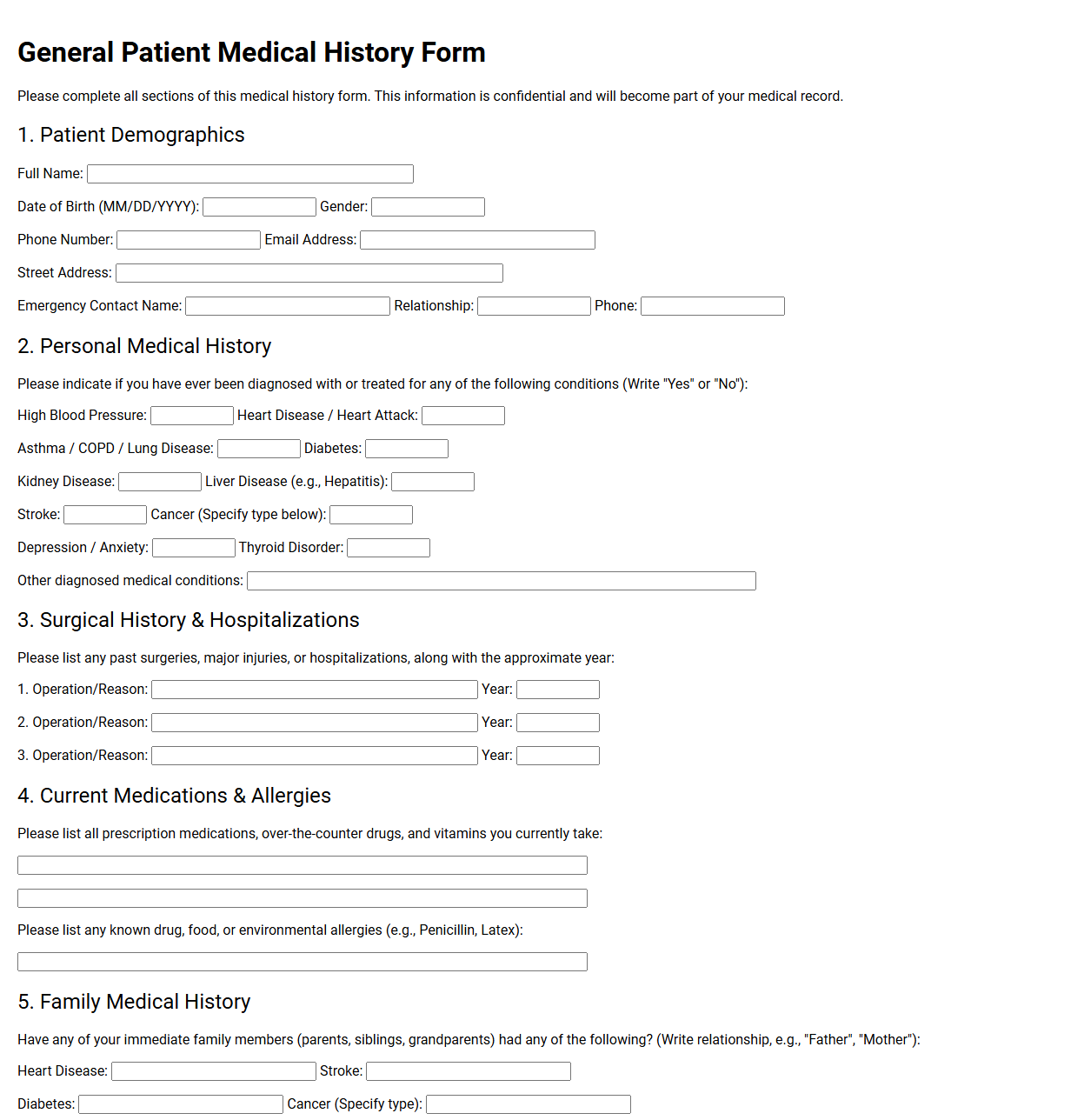
General Patient Medical History Form
💾 General Patient Medical History Form .pdf
A general patient medical history form gathers vital health data before any treatment. This standard document records past diagnoses, surgeries, active medications, allergies, and family health backgrounds. Collecting this information helps healthcare providers assess risks, avoid drug interactions, and deliver safe, personalized care tailored to each patient's unique clinical profile.
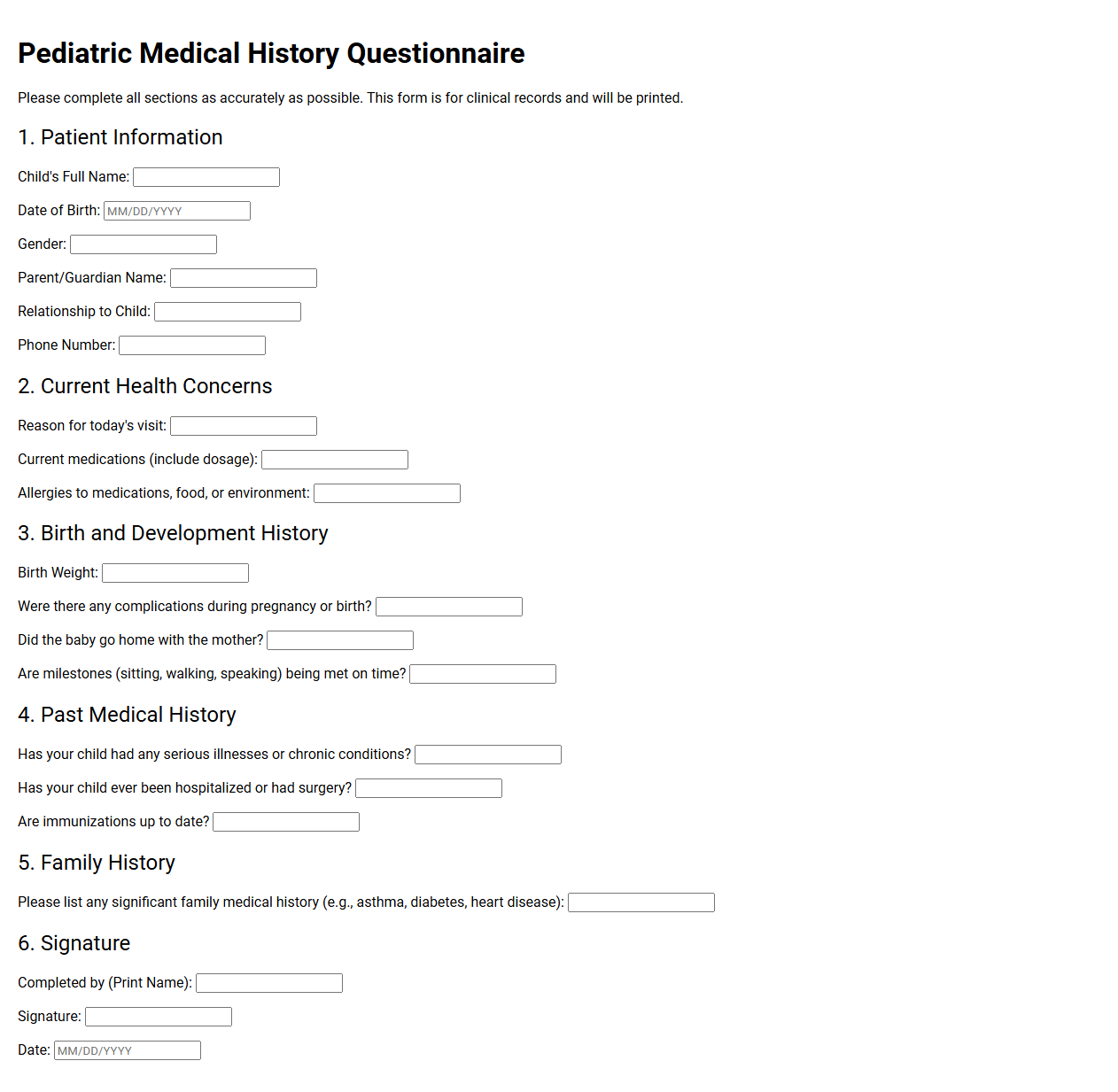
Pediatric Medical History Questionnaire
💾 Pediatric Medical History Questionnaire .pdf
A pediatric medical history questionnaire gathers vital health information about a child from birth to the present. This document typically records immunization histories, developmental milestones, past illnesses, surgeries, allergies, and family genetic conditions. It helps pediatricians thoroughly understand the patient's background to provide safe, personalized, and highly effective healthcare.
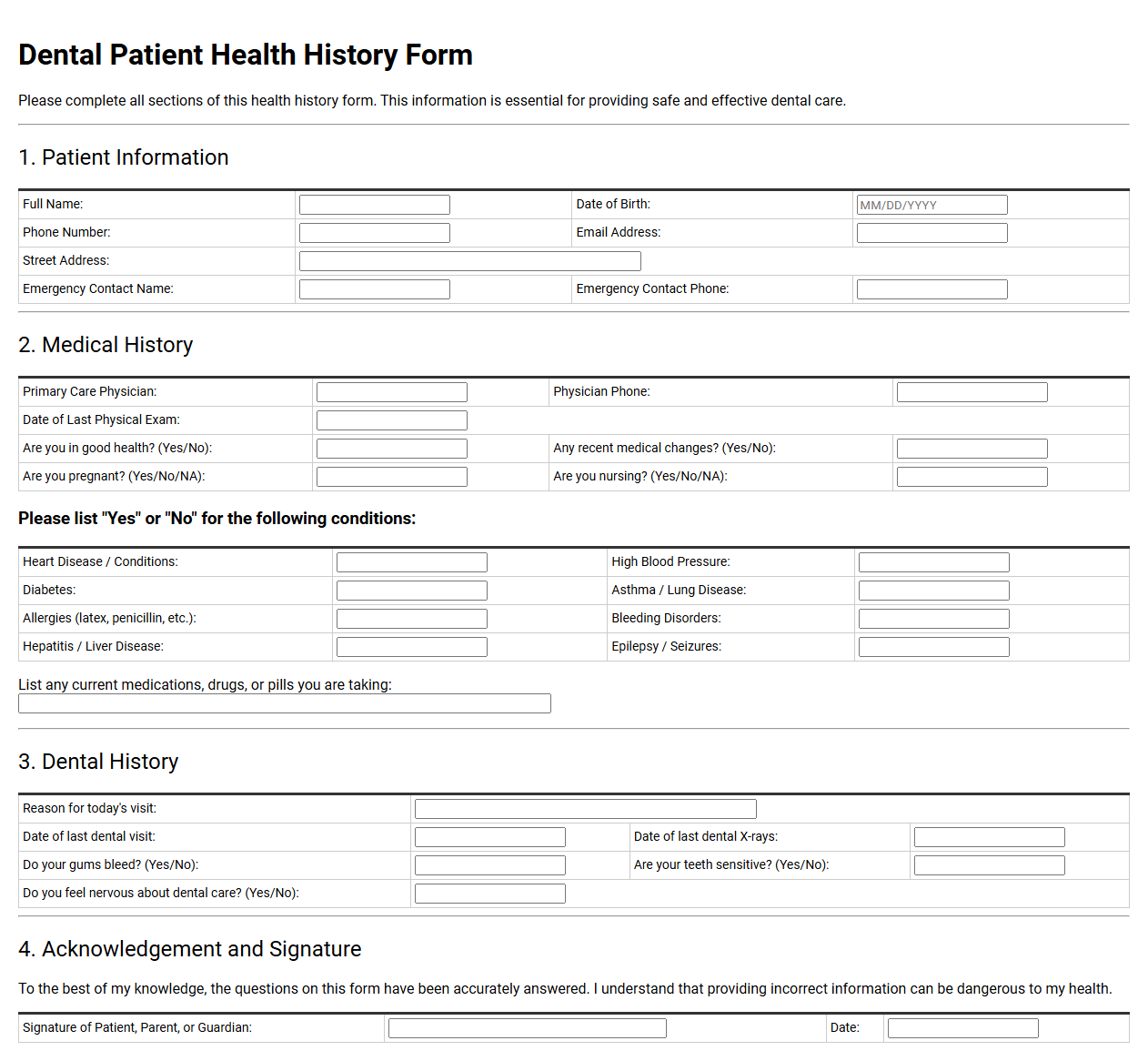
Dental Patient Health History Form
💾 Dental Patient Health History Form .pdf
A dental patient health history form gathers crucial medical information before treatment begins. It records past surgeries, current medications, allergies, and chronic conditions like diabetes or heart disease. Dentists utilize this data to customize treatment plans safely, avoiding adverse drug interactions and ensuring complete patient safety during all clinical procedures.
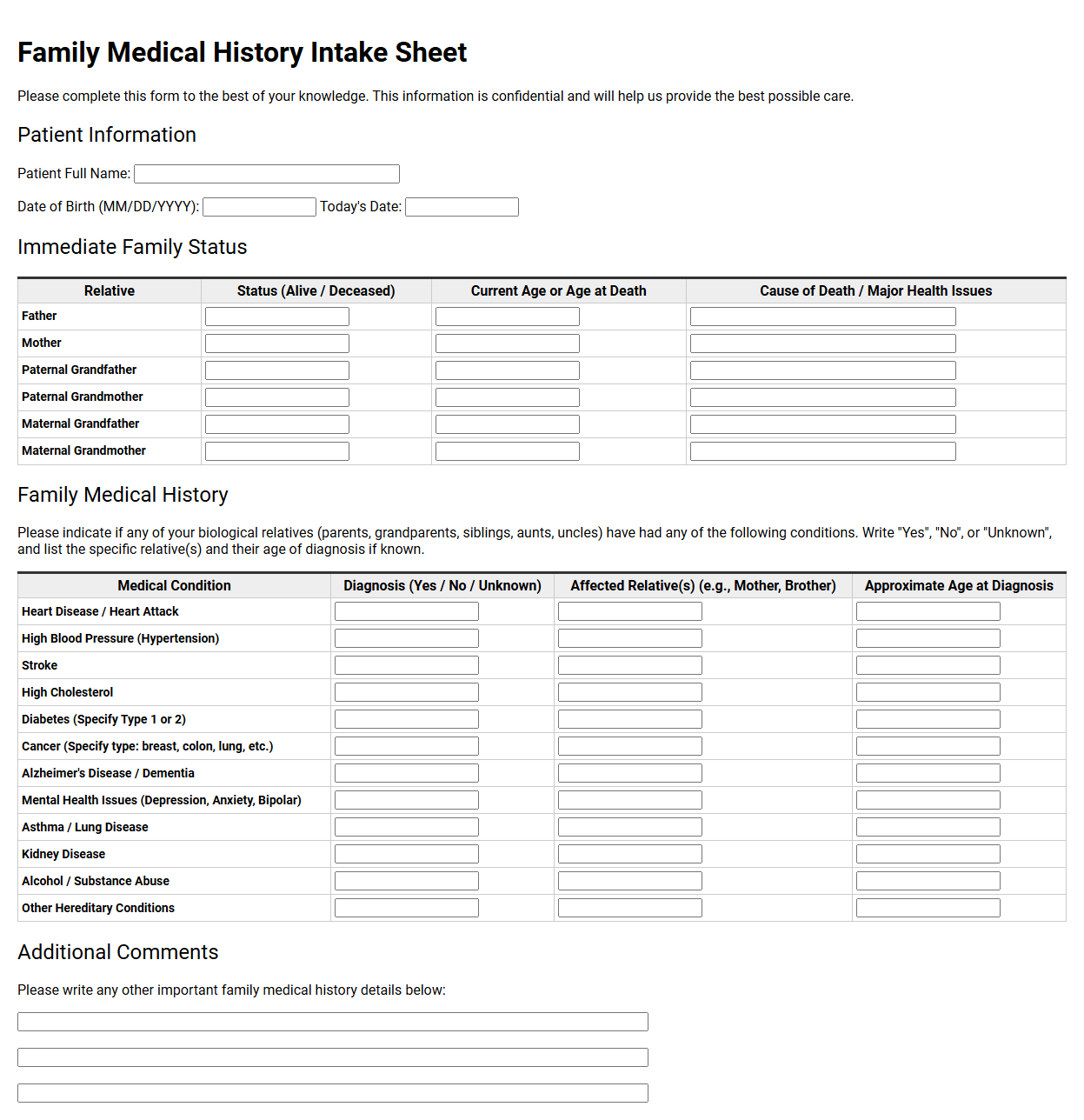
Family Medical History Intake Sheet
💾 Family Medical History Intake Sheet .pdf
A family medical history intake sheet compiles multi-generational health data to help clinicians assess hereditary risks. Patients record chronic conditions, cardiovascular events, and cancers among close relatives. This comprehensive record guides personalized preventive care, aids in accurate diagnoses, and informs future screening schedules during routine medical consultations.
Patient Past Surgical History Record
💾 Patient Past Surgical History Record .pdf
A patient's past surgical history record compiles all prior operative procedures, chronicling dates, anatomical sites, and specific indications. This clinical document details anesthesia reactions and implant details, guiding healthcare providers in making safe, informed decisions for upcoming treatments, minimizing redundant diagnostics, and optimizing perioperative care strategies.
Chronic Illness and Medication Questionnaire
💾 Chronic Illness and Medication Questionnaire .pdf
A chronic illness and medication questionnaire helps healthcare providers gather vital health data. This document collects details on long-term conditions, current prescriptions, dosages, and daily symptoms. By tracking this information, doctors can customize treatment plans, prevent harmful drug interactions, and monitor your ongoing wellness journey effectively.
Patient Allergy and Medication History Form
💾 Patient Allergy and Medication History Form .pdf
A patient allergy and medication history form collects critical health data before treatment. It records current prescriptions, over-the-counter drugs, and herbal supplements. Additionally, it documents known adverse reactions to substances, foods, or environmental triggers, ensuring healthcare providers administer safe treatments and avoid dangerous drug interactions during care.
New Patient Health Intake Questionnaire
💾 New Patient Health Intake Questionnaire .pdf
A new patient health intake questionnaire gathers crucial medical history, contact details, and lifestyle habits. This foundational document helps healthcare providers understand your background, identify potential risks, and design personalized treatment plans. Patients typically complete it before their first appointment to ensure safe, efficient, and comprehensive clinical care.
Cardiovascular Risk Assessment Questionnaire
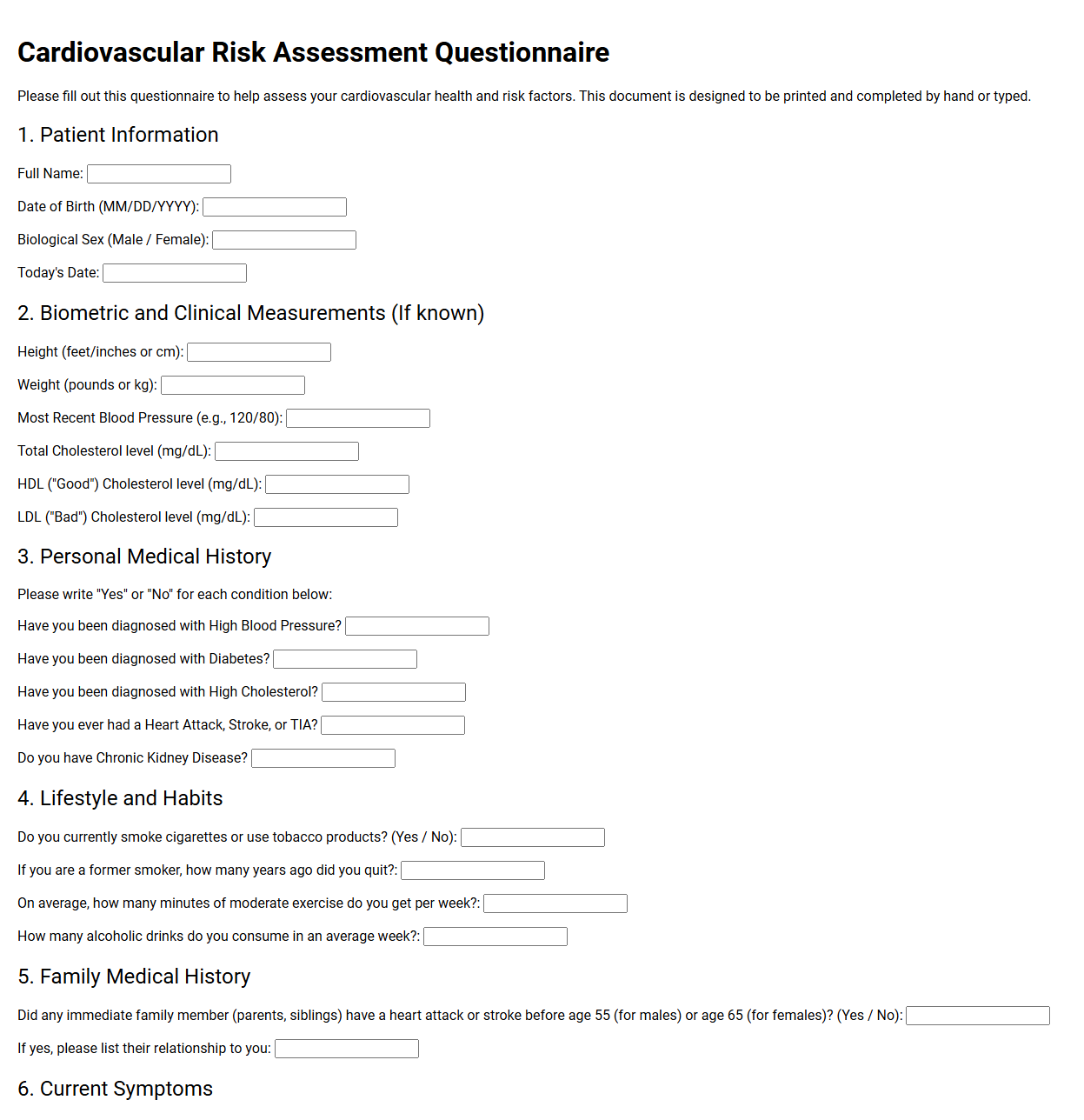
💾 Cardiovascular Risk Assessment Questionnaire .pdf
A cardiovascular risk assessment questionnaire is a vital medical tool used to evaluate a patient's heart health. This document gathers data on lifestyle choices, family medical history, smoking habits, and existing conditions. Healthcare providers analyze these responses to estimate the probability of future cardiac events and design personalized prevention strategies.
Prenatal Health History Assessment Form
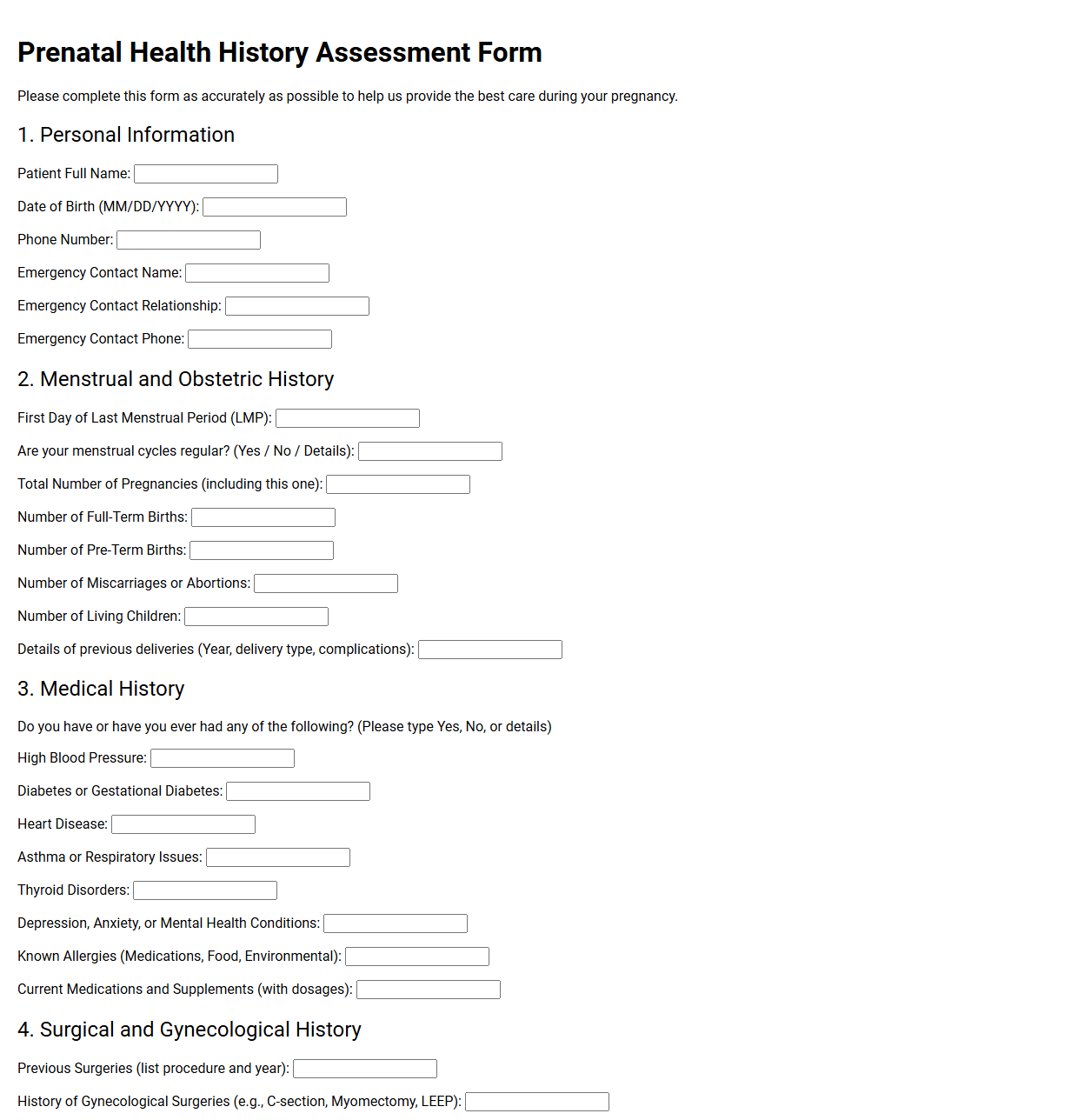
💾 Prenatal Health History Assessment Form .pdf
A prenatal health history assessment form is a foundational intake document used by obstetric providers to compile comprehensive medical backgrounds. It systematically records maternal health conditions, previous pregnancies, genetic risks, and lifestyle factors. This detailed profile guides clinicians in identifying potential complications and establishing personalized care plans for maternal and fetal well-being.
Mental Health Intake Questionnaire
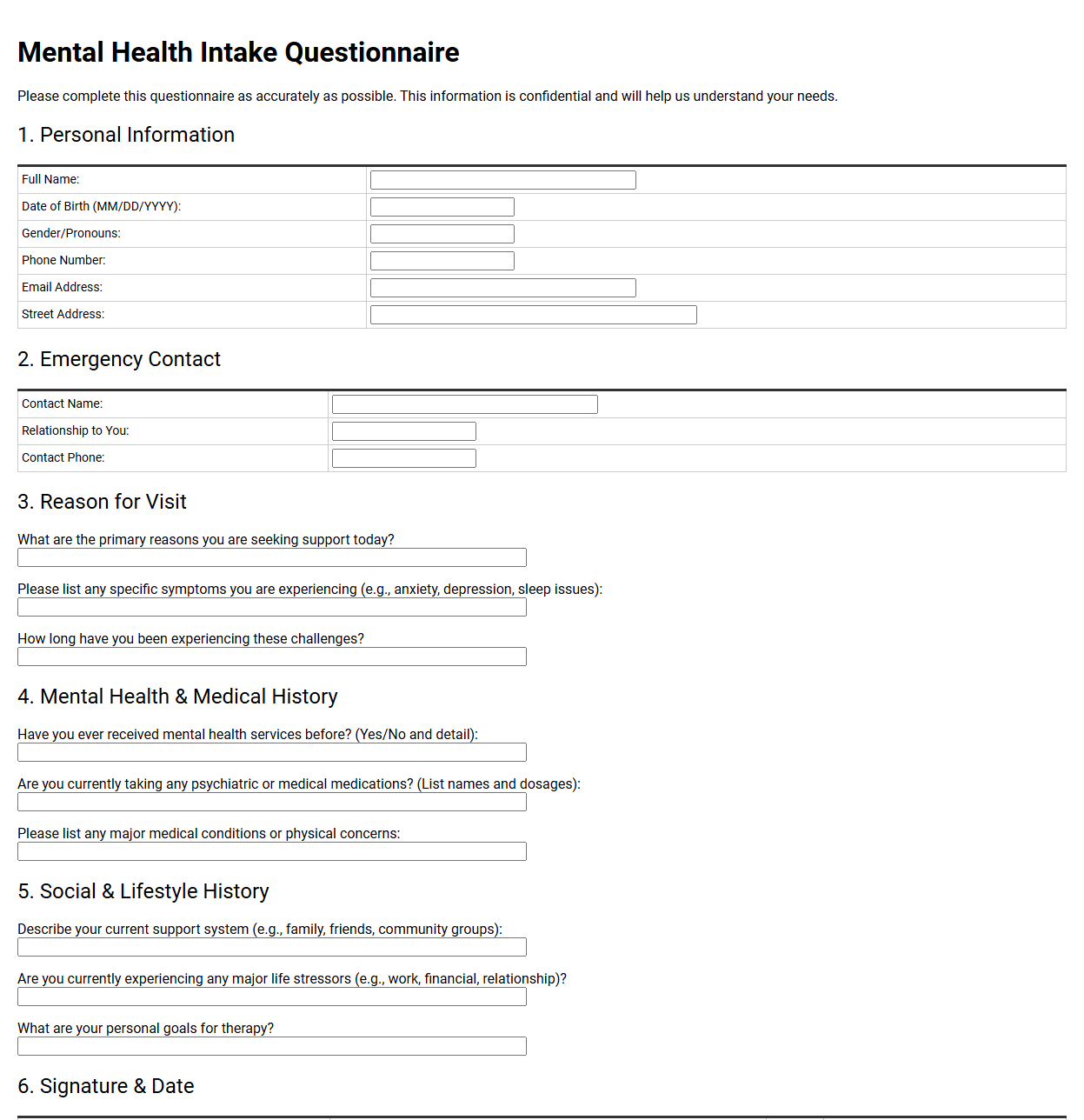
💾 Mental Health Intake Questionnaire .pdf
A mental health intake questionnaire gathers crucial background information before therapy begins. This document collects personal history, current symptoms, lifestyle habits, and medical records. It helps clinicians understand your unique needs, enabling them to design an effective, personalized treatment plan. Completing it honestly ensures a safe and productive therapeutic journey.
Patient Lifestyle and Social History Form
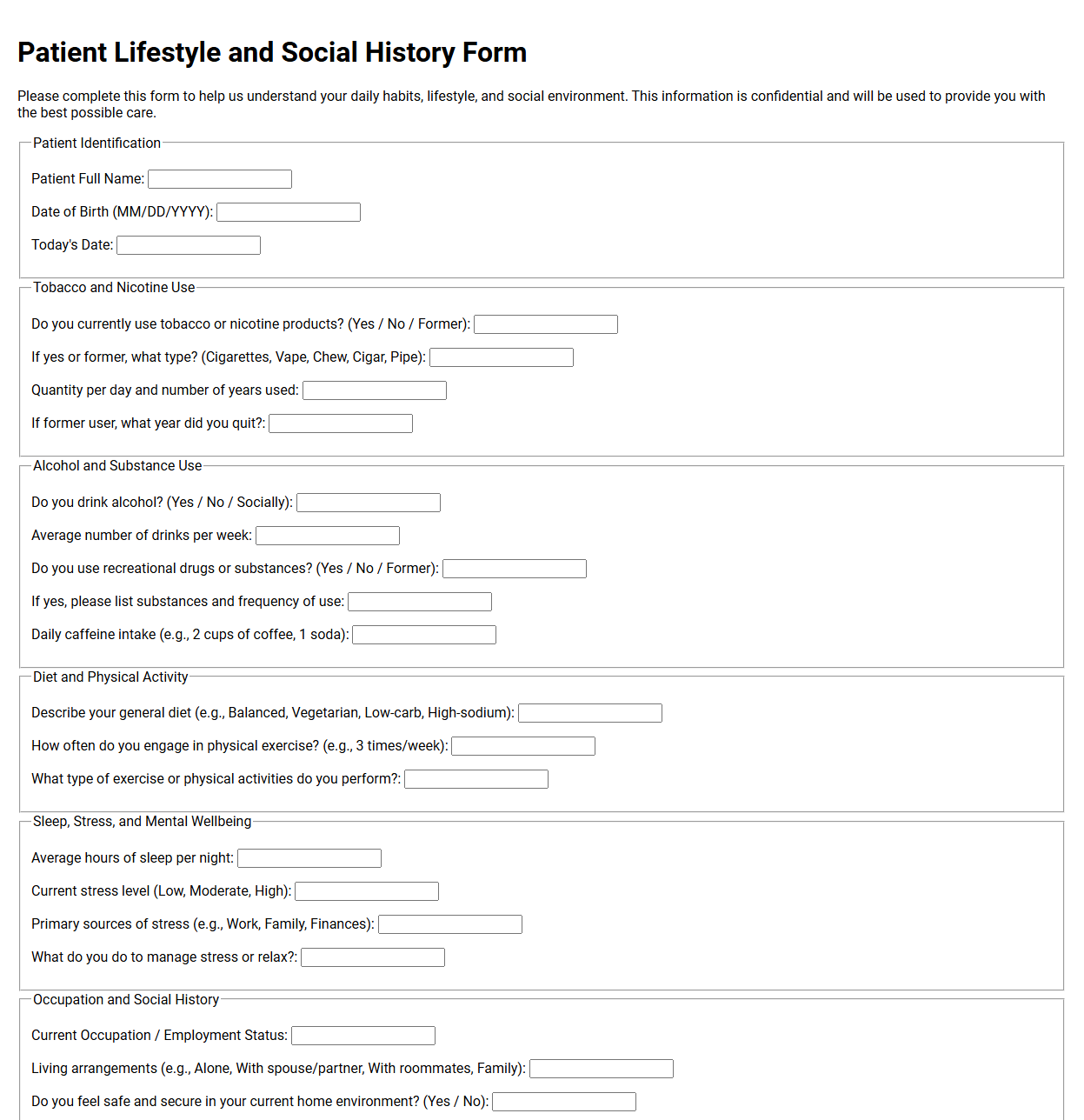
💾 Patient Lifestyle and Social History Form .pdf
A patient lifestyle and social history form collects critical data regarding daily habits and background. It documents dietary choices, exercise routines, sleep patterns, and substance use. Additionally, it records occupational hazards, living arrangements, and support systems. This information helps healthcare providers tailor personalized treatment plans and assess overall wellness risks.
Geriatric Patient Health History Questionnaire
💾 Geriatric Patient Health History Questionnaire .pdf
A geriatric patient health history questionnaire gathers comprehensive information regarding an older adult's medical background. This document typically details past diagnoses, current medications, surgeries, family history, and lifestyle habits. It also assesses cognitive function, mobility, and daily living support, helping healthcare providers deliver tailored, safe, and effective geriatric care.
Patient Immunization and Vaccination History Form
💾 Patient Immunization and Vaccination History Form .pdf
A patient immunization and vaccination history form compiles a person's complete inoculation record. This crucial document tracks past vaccines, administration dates, dosages, and healthcare providers. Clinics use this information to identify missing immunizations, ensure overall public health safety, and facilitate accurate medical planning during routine checkups or emergency care visits.
Post-Operative Medical History Questionnaire
💾 Post-Operative Medical History Questionnaire .pdf
A post-operative medical history questionnaire is a vital clinical document used to track a patient's recovery progress. It gathers detailed information regarding pain levels, wound healing, medication adherence, and any unexpected symptoms. This record helps healthcare providers monitor recovery, identify potential complications early, and customize ongoing rehabilitation plans.
Patient Medical History Questionnaire FAQ
Why is a comprehensive patient medical history questionnaire essential for clinical care?
This form provides healthcare providers with a holistic view of a patient's health background. By documenting past diagnoses, surgeries, allergies, and chronic conditions, clinicians can make highly informed diagnostic decisions, avoid dangerous drug interactions, and customize treatment plans tailored to the patient's unique physiological profile.
What is the significance of the family medical history section in this questionnaire?
Family medical history reveals genetic predispositions to hereditary conditions like cardiovascular disease, diabetes, or certain cancers. Capturing this data allows practitioners to implement early screenings, recommend preventative lifestyle modifications, and identify potential health risks before they manifest clinically, significantly improving long-term patient health outcomes.
How do lifestyle and social history questions contribute to patient assessment?
Questions regarding diet, exercise, alcohol consumption, smoking, and occupational hazards illuminate environmental factors influencing health. This information helps clinicians identify behavioral risks, contextualize current physical symptoms, and design practical wellness interventions that align with the patient's daily habits and social environment.
Why must the questionnaire meticulously document current medications and allergies?
Tracking active prescriptions, over-the-counter drugs, and supplements prevents adverse drug-to-drug interactions. Simultaneously, documenting specific allergies to medications, foods, or environmental triggers is crucial for patient safety, ensuring providers do not prescribe contraindicated therapies or administer substances that could provoke life-threatening allergic reactions.
What is the role of the "Review of Systems" portion in this health questionnaire?
The Review of Systems is a systematic sweep of different body systems to identify active symptoms the patient might otherwise forget to mention. It helps uncover hidden clinical issues, guides the physical examination, and ensures no subjective physical complaints are overlooked during the initial patient evaluation.
Disclaimer:
The documents and templates provided on this page are for informational and illustrative purposes only. They do not constitute professional, legal, or financial advice, and should not be relied upon as such. Because individual circumstances and regulatory requirements vary, these materials may not be suitable for your specific needs. We recommend consulting with a qualified professional before adapting or using any of these examples for official or commercial purposes.